Abstract
- The da Vinci SP system has been increasingly used in several surgical fields, partly because it can reduce the number of abdominal incisions by enabling surgery through a single access port. However, single-incision laparoscopic splenectomy is technically demanding because of the spleen’s anatomical position and vascularity, and significant bleeding may occur without meticulous hilar and perisplenic dissection. This report describes a robotic splenectomy performed with the da Vinci SP system using a single-port-plus-one approach. A single umbilical access port was placed through an approximately 3-cm incision, and an additional trocar was inserted in the left abdomen for use by the assistant, including introduction of energy devices, a laparoscopic stapler, and a drain. We present a representative case treated using this approach. The patient was a 42-year-old woman with hemolytic anemia, hyperbilirubinemia, a body mass index of 24.2 kg/m2, and splenomegaly measuring 15.1 cm in maximal craniocaudal diameter. The console time was 100 minutes, and the estimated blood loss was 10 mL. The splenic hilum was divided using a laparoscopic stapler. No surgical complications occurred, and the patient was discharged on postoperative day 3. Robotic splenectomy using the da Vinci SP system with an additional assistant trocar was technically feasible in this carefully selected patient. Further studies are needed to determine its safety, indications, and comparative advantages over conventional laparoscopic or multiport robotic approaches.
-
Keywords: Splenectomy, Robotic surgical procedures, Laparoscopy, Minimally invasive surgical procedures
Introduction
Laparoscopic splenectomy is the standard approach for elective splenectomy offering less postoperative pain, shorter hospital stay, and improved cosmetic outcomes compared with open surgery [1,2]. Conventional multiport laparoscopic splenectomy is most commonly performed, while reduced-port and single-incision laparoscopic surgery (SILS) have been introduced to further minimize access trauma [3]. Although single-port splenectomy may improve cosmesis and reduce wound-related morbidity, it remains limited by restricted instrument articulation, instrument crowding, and suboptimal ergonomics [4].
Robotic splenectomy using multiport platforms has been adopted in select centers to improve dexterity, tremor filtration, and three-dimensional visualization. However, multiport robotic approaches still require multiple incisions, potentially reducing cosmetic advantages and increasing port-site morbidity. Recently, single-incision and single+1 (which refers to “single-incision with an additional trocar”) robotic strategies have gained attention for reducing invasiveness while maintaining robotic precision [5-8]. The da Vinci SP (Single Port) system was designed for single-site surgery and incorporates a flexible 25-mm cannula accommodating a wristed camera and three articulating instruments through a single access point. This architecture enables improved triangulation, ergonomics, and visualization in confined spaces for splenic surgery. With an auxiliary 12-mm port (“Single+1”), the assistant can introduce energy devices, suction, staplers, or retractors without negating the minimally invasive intent.
Reports of SP-based splenectomy remain scarce [9]. To our knowledge, descriptions of technical modifications and outcomes of single+1 port robotic splenectomy using the SP platform are limited. We describe our single+1 port robotic splenectomy technique using the da Vinci SP system and provide early insight into its feasibility, safety, and potential limitations for benign splenic disease.
The study was approved by the Institutional Review Board (IRB) of our institution (IRB approval no. 2025-07-078), and the requirement for informed consent was waived due to the retrospective nature of the study.
Case Presentation
Patient information
A 42-year-old woman with progressive left upper-quadrant discomfort and jaundice. She had been diagnosed with hemolytic anemia 10 years earlier without definitive therapy. Her body mass index was 24.2 kg/m2, with no significant comorbidities. Laboratory tests showed hyperbilirubinemia (total bilirubin, 3.53 mg/dL) and mild anemia (hemoglobin, 11.9 g/dL). Contrast-enhanced computed tomography demonstrated splenomegaly, with a maximal craniocaudal diameter of 15.1 cm. A single+1 port robotic splenectomy using the da Vinci SP system (Intuitive Surgical) was planned (January 14, 2025).
Surgical technique
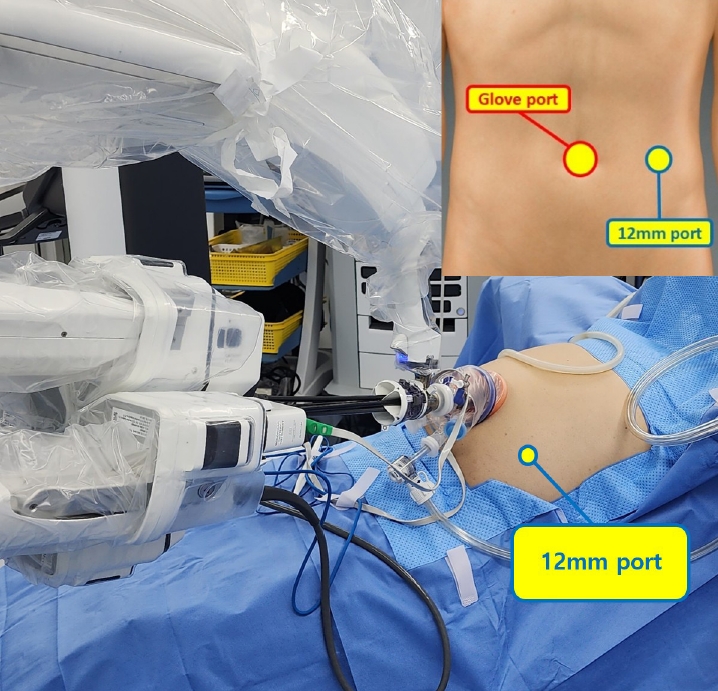
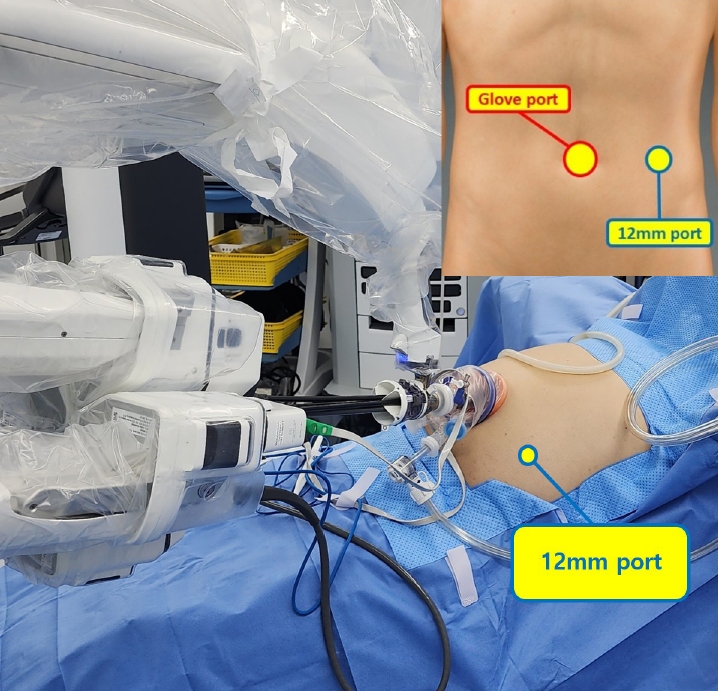
Under general anesthesia, the patient was placed supine. A 2.5-cm transumbilical incision was made, and a Glove port (Nelis Corp.) was inserted. The SP trocar was introduced through the port for docking. A 12-mm assistant port was placed at the level of the umbilicus along the left midclavicular line for assistant-driven instruments (energy device, suction, stapler, etc.) (Fig. 1).
The procedure followed these steps: (1) docking and positioning; (2) division of the left gastrocolic ligament with ligation/transection of accessory splenic vessels and left gastroepiploic vessels; (3) division of short gastric vessels and the gastrosplenic ligament; (4) dissection along the inferior border of the pancreas with division of the splenocolic ligament and control of splenic vessel branches; (5) isolation and stapled division of the splenic hilum; (6) division of the splenorenal and splenophrenic ligaments; and (7) hemostasis and specimen retrieval.
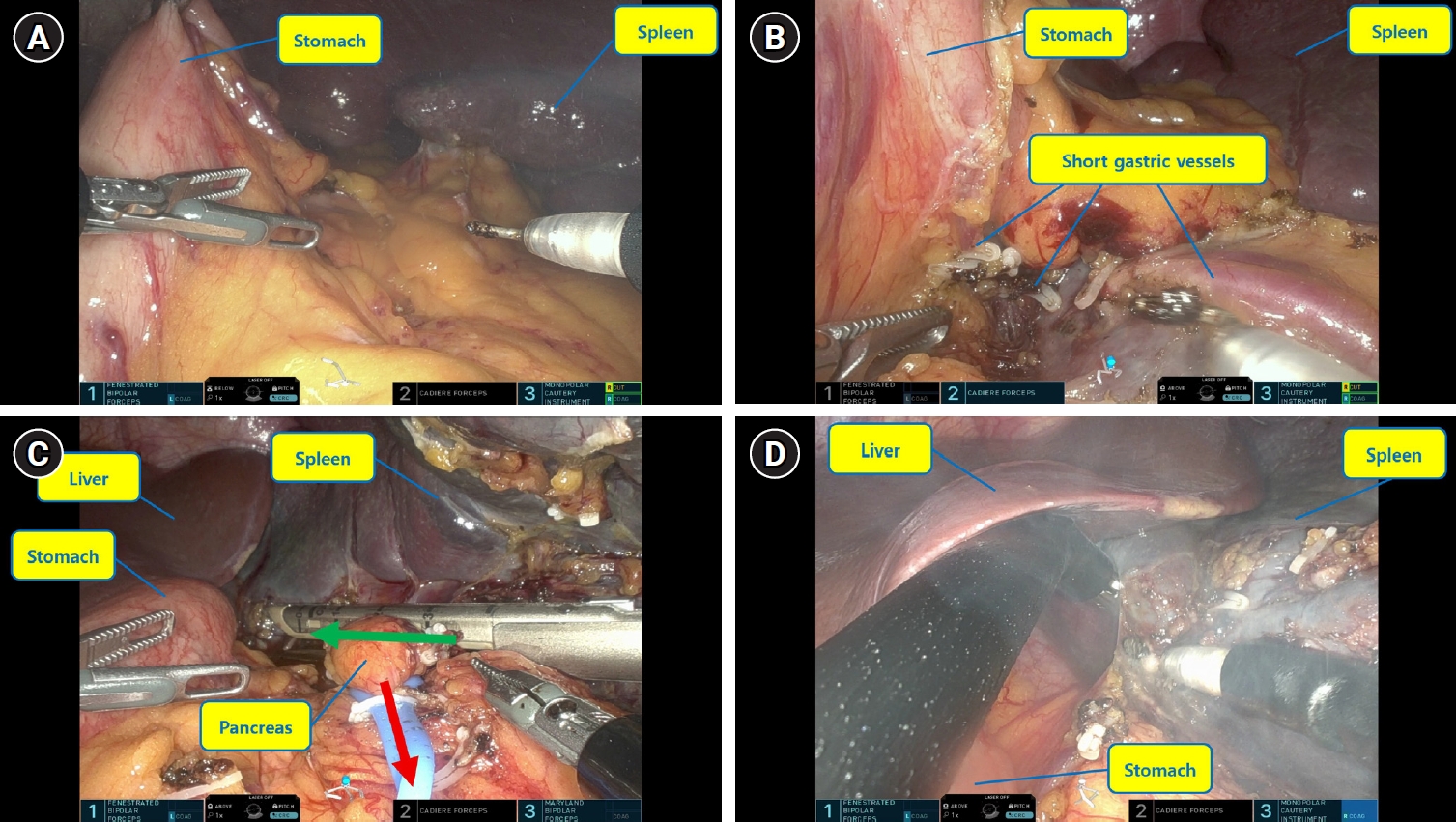
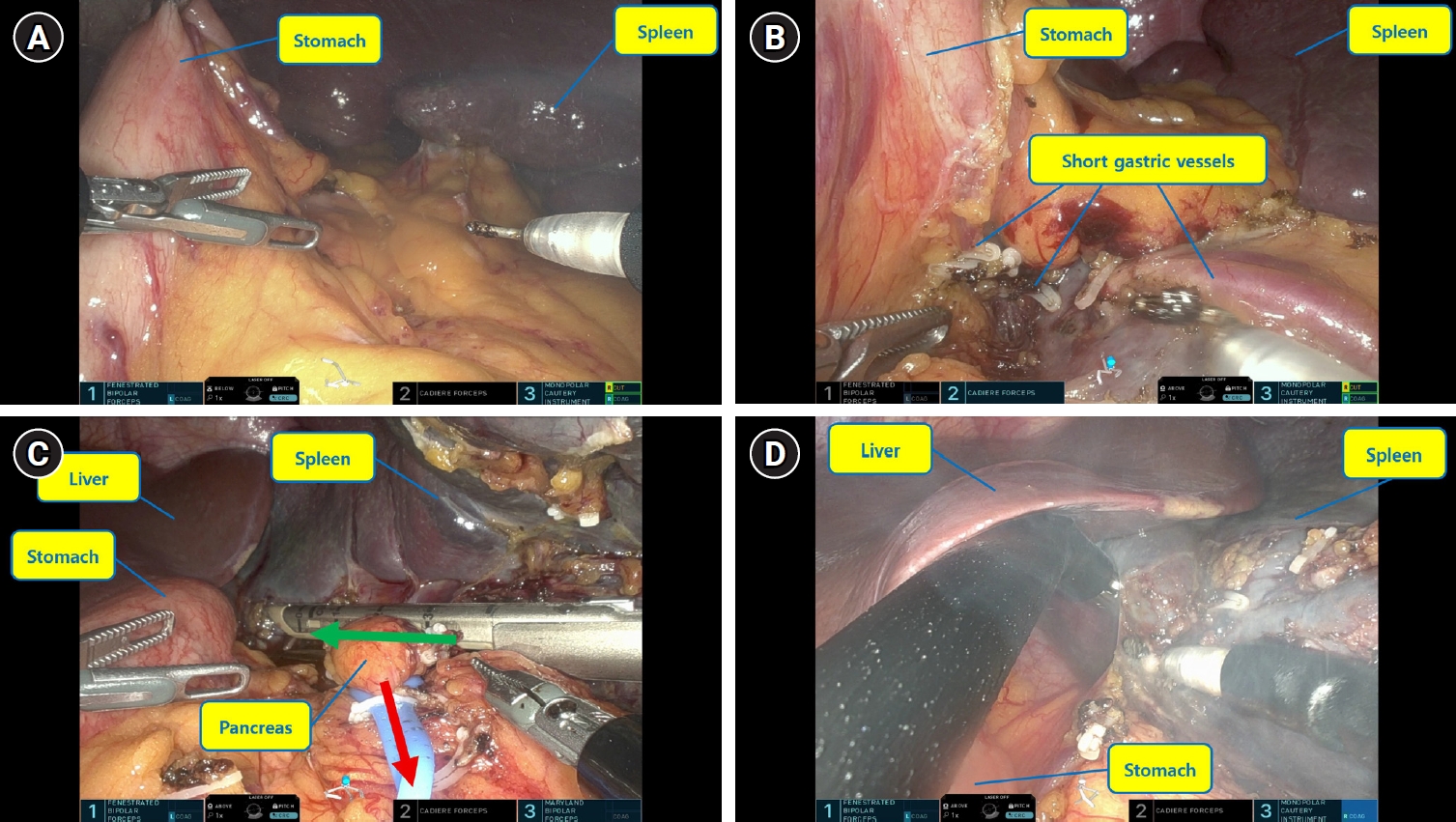
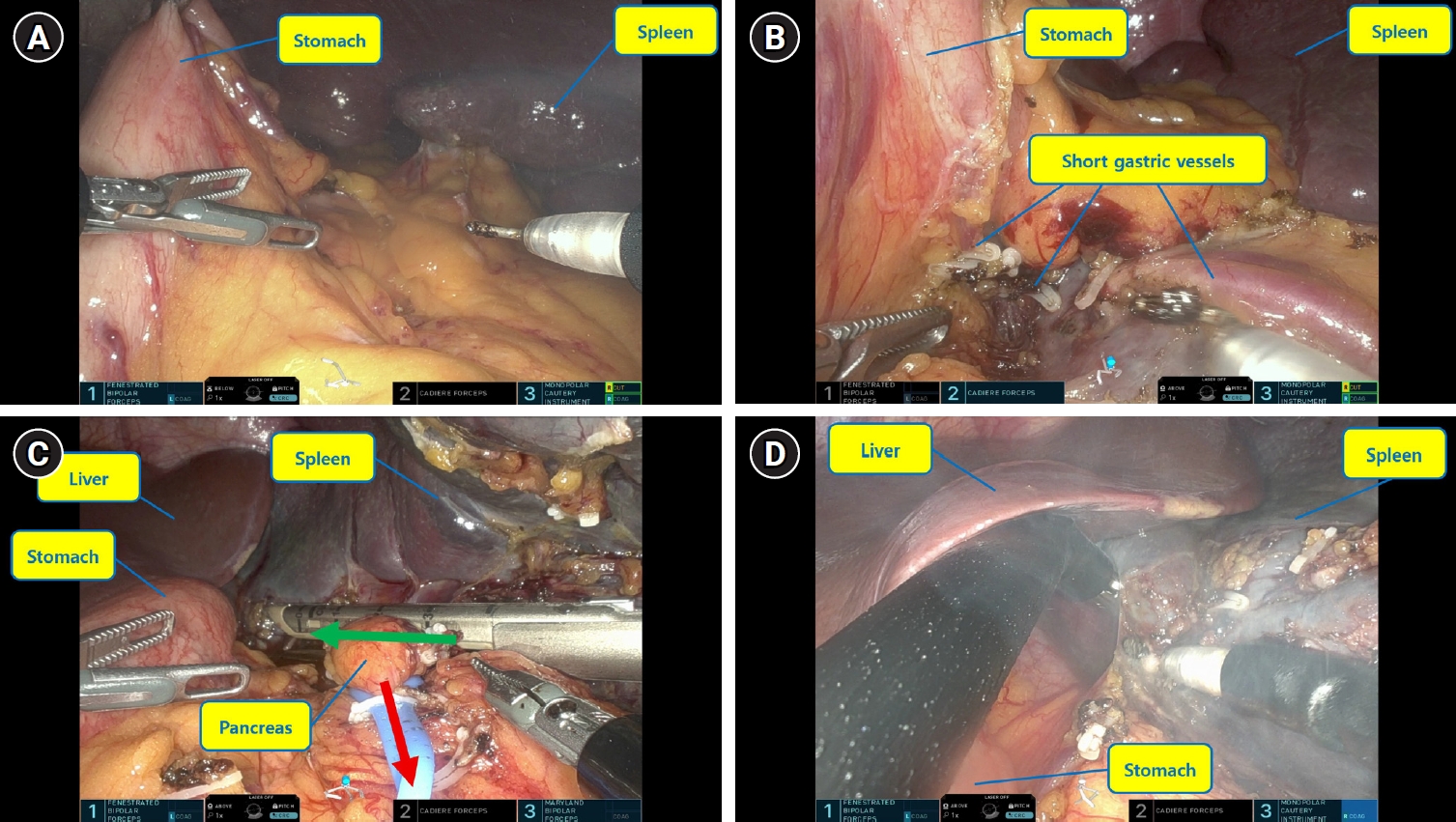
For steps 1 and 2, instruments were configured with a monopolar hook (3 o’clock), fenestrated bipolar forceps (9 o’clock), and Cadiere forceps (12 o’clock). The stomach was elevated sequentially (anterior then posterior wall) to expose the gastrocolic ligament and enable safe progression (Fig. 2A).
Beginning with step 3, the Cadiere forceps were repositioned to the 6 o’clock arm to improve retraction and ergonomics. Instrument selection for the 3 and 9 o’clock arms (monopolar hook, bipolar forceps, Maryland bipolar, polymer clip applier) was adjusted according to operative needs. At this stage, the stomach was retracted using the 9 o’clock arm, the gastrosplenic ligament and short gastric vessels were divided (Fig. 2B). For step 4, the pancreas or spleen was retracted using the 6 and 9 o’clock arms to secure the operative field. During step 5, isolation of the splenic hilum was facilitated, when necessary, by looping a rubber vessel loop around the hilum and retracting it. Division of the hilum was performed by the assistant through the 12-mm port using a laparoscopic linear stapler (Fig. 2C). For steps 5 and 6, adequate visualization was achieved by retracting the stomach or liver using the 9 o’clock arm (Fig. 2D). In cases where dense visceral fat or anatomical variations limited visibility, the assistant surgeon utilized the 12-mm additional port to insert a laparoscopic instrument to assist with exposure.
Total operative time was 150 minutes and console time was 100 minutes. Estimated blood loss was 10 mL, and the resected spleen weighed 232 g. There was no intraoperative conversion. The patient was discharged on postoperative day 3. No postoperative complications occurred, including no events of Clavien–Dindo grade II or higher and no postoperative pancreatic fistula requiring intervention. No transfusion was required. Postoperative vaccination was provided per institutional protocol.
Discussion
Robotic splenectomy is a valuable alternative to conventional laparoscopic approaches, offering enhanced visualization and instrument articulation. However, single-incision laparoscopic splenectomy is often constrained by instrument collision, limited triangulation, and unfavorable ergonomics, particularly around the splenic hilum. Multiport robotic platforms mitigate some of these issues but still require multiple incisions. The da Vinci SP system provides a single-site robotic platform capable of deploying a wristed camera and multiple articulating instruments through one access point, potentially improving dexterity and visualization while minimizing access trauma.
In this case, the SP system enabled stable visualization and precise dissection in a confined workspace, including safe vessel handling around the hilum. The single+1 modification was key. The auxiliary 12-mm port allowed the assistant to use suction, energy devices, staplers, and retractors, improving exposure and efficiency without compromising the minimally invasive intent. This approach may address limitations of single-site surgery, particularly in patients with visceral adiposity or complex vascular anatomy.
Compared with conventional laparoscopic splenectomy, this approach may offer improved ergonomics, stable three-dimensional visualization, and wristed articulation during dissection around the short gastric vessels and splenic hilum. Instrument collision, a limitation of conventional SILS, was not a major issue in this case because the da Vinci SP system allows articulating instruments to be deployed through a dedicated single-port cannula, while the auxiliary trocar permits independent assistant-driven suction, retraction, energy-device use, and stapler insertion. However, conventional laparoscopic splenectomy remains the standard approach in most centers because of its established safety, lower cost, wide availability, and shorter setup requirements. Compared with multiport robotic splenectomy using the da Vinci Xi system, the SP approach with an additional trocar may reduce the number of abdominal incisions, but it has several technical disadvantages, including less freedom for instrument spacing and retraction, potentially more limited exposure in challenging cases, and the lack of a dedicated robotic energy device within the SP platform. Therefore, laparoscopic energy devices or other assistant-driven instruments may be required through the auxiliary trocar. These limitations may become more relevant in patients with marked splenomegaly, visceral obesity, severe adhesions, or complex hilar anatomy. Thus, this technique should be regarded as a reduced-port strategy that balances minimal access trauma with the safety and practicality of assistant-driven maneuvers, and careful patient selection remains essential.
In conclusion, robotic splenectomy using the da Vinci SP system with an additional trocar was technically feasible in this carefully selected patient with benign splenic disease. Because this report describes a single case, the safety and effectiveness of this technique should be interpreted cautiously. Further prospective studies with larger cohorts are needed to clarify appropriate indications, technical limitations, learning curves, and comparative outcomes, including long-term results, incisional hernia rates, and patient-reported satisfaction.
Disclosure
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization: YJ, SKM; Data curation: YJ; Formal analysis: YJ; Investigation: YJ; Methodology: YJ, SKM; Project administration: SKM; Resources: YS; Supervision: SKM; Visualization: YS; Writing–original draft: YJ; Writing–review & editing: YJ, SKM.
Fig. 1.Operative setup and port placement for robotic splenectomy using the da Vinci SP system with an additional assistant trocar. The da Vinci SP trocar was inserted through a 2.5-cm transumbilical incision using a Glove port, and a 12-mm assistant trocar was placed on the left midclavicular line at the level of the umbilicus. The inset schematic shows the relative positions of the umbilical SP access port and the auxiliary assistant trocar.
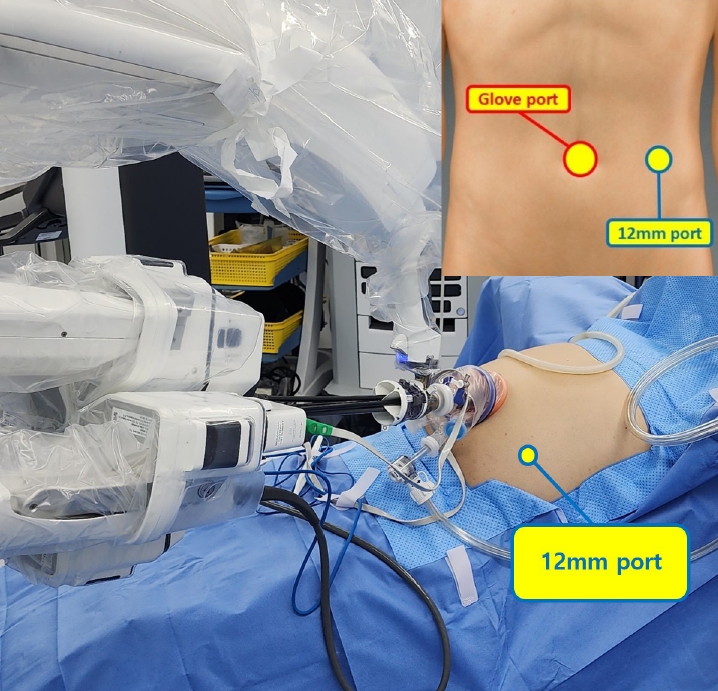
Fig. 2.(A) Exposure of the gastrocolic ligament. The stomach was sequentially elevated by grasping the anterior and posterior walls with Cadiere forceps to expose the gastrocolic ligament. (B) Division of the gastrosplenic ligament and short gastric vessels. The stomach was retracted using the 9-o’clock arm, and the short gastric vessels and gastrosplenic ligament were divided. (C) Isolation and stapled division of the splenic hilum. The splenic hilum was encircled with a rubber vessel loop to facilitate traction and define the stapling line. A laparoscopic linear stapler was introduced through the 12-mm assistant port toward the splenic hilum, as indicated by the arrow, and the hilum was divided under direct robotic visualization. (D) Exposure during the later phase of splenic mobilization. Adequate visualization was achieved by retracting the stomach or liver using the 9-o’clock arm.
REFERENCES
- 1. Katkhouda N, Hurwitz MB, Rivera RT, Chandra M, Waldrep DJ, Gugenheim J, et al. Laparoscopic splenectomy: outcome and efficacy in 103 consecutive patients. Ann Surg. 1998;228:568-578.ArticlePubMedPMC
- 2. Sampath S, Meneghetti AT, MacFarlane JK, Nguyen NH, Benny WB, Panton ON. An 18-year review of open and laparoscopic splenectomy for idiopathic thrombocytopenic purpura. Am J Surg. 2007;193:580-584.ArticlePubMed
- 3. Vatansev C, Ece I Jr. Single incision laparoscopic splenectomy with double port. Surg Laparosc Endosc Percutan Tech. 2009;19:e225-e227.ArticlePubMed
- 4. Lagrand R, Kehdy F. Laparoendoscopic single site splenectomy. Am Surg. 2010;76:E158-E159.ArticlePubMedPDF
- 5. Chong JU, Lee JY, Lim JH. Early experiences in robotic single-site plus one port platform for complex hepatobiliary and pancreatic surgery. Int J Med Robot. 2024;20:e2602.ArticlePDF
- 6. Jang EJ, Kim KW. Exploring the potential of robotic single-port surgery for gallbladder cancer: initial insights and future prospects. Ann Surg Oncol. 2025;32:440-442.ArticlePubMedPDF
- 7. Na YH, Kim WB, Kang JS, Choi SB, Kim WJ. Early outcomes of single-port robotic left lateral sectionectomy in patients with hepatic tumor. Ann Surg Treat Res. 2024;106:78-84.ArticlePubMedPMCPDF
- 8. Kim SH, Kim NR, Kang CM. Robotic single-port plus one-port splenic vessel-conserving spleen-preserving distal pancreatectomy: a case report. J Minim Invasive Surg. 2024;27:177-180.ArticlePubMedPMC
- 9. Klazura G, Sims T, Rojnica M, Koo N, Lobe T. Single port robotic splenectomy for pyruvate kinase deficiency in a five-year-old patient, a case report of a surgical first. Int J Surg Case Rep. 2021;84:106122.ArticlePubMedPMC
Citations
Citations to this article as recorded by


 , Seog Ki Min
, Seog Ki Min
 PubReader
PubReader ePub Link
ePub Link Cite this Article
Cite this Article