
Articles
- Page Path
- HOME > J Surg Innov Educ > Volume 3(1); 2026 > Article
-
Original Article
Artificial Intelligence-Assisted Monitoring for Detecting Perioperative Safety Deviations in General Surgical Practice -
Opeyemi Qozeem Asafa1
 , Aishat Omowunmi Asafa2, Ayodeji Olaolu Oyeniran1, Olajide Emmanuel Babalola3, Olumuyiwa Tope Ajayeoba1, Roseline Olufunmilola Folami4, Ganiyu Adebukola Oyeniyi1, Kehinde Adesola Alatishe5, Adegboyega Segun Afolabi1, Ismail Idowu Uthman1
, Aishat Omowunmi Asafa2, Ayodeji Olaolu Oyeniran1, Olajide Emmanuel Babalola3, Olumuyiwa Tope Ajayeoba1, Roseline Olufunmilola Folami4, Ganiyu Adebukola Oyeniyi1, Kehinde Adesola Alatishe5, Adegboyega Segun Afolabi1, Ismail Idowu Uthman1 -
Journal of Surgical Innovation and Education 2026;3(1):14-28.
DOI: https://doi.org/10.69474/jsie.2026.00080
Published online: June 15, 2026
1Department of Surgery, UNIOSUN Teaching Hospital, Osogbo, Nigeria
2Department of Nursing, Westley Guild, Ilesha, Nigeria
3Department of Obstetrics & Gynaecology, Obafemi Awolowo University, Ile-Ife, Nigeria
4Department of Nursing, Osun State University, Osogbo, Nigeria
5Departement of Orthopaedic and Traumatology, National Orthopaedics Hospital, Igbobi, Nigeria
- Corresponding author: Opeyemi Qozeem Asafa, FWACs Department of Surgery, UNIOSUN Teaching Hospital, P.M.B. 5000, Osogbo, Osun State, Nigeria Tel: +234-8036250105, E-mail: solution238@yahoo.com
© 2026 Korean Surgical Skill Study Group
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 258 Views
- 9 Download
Abstract
-
Background
- Perioperative safety deviations remain an important challenge in surgical care despite implementation of safety measures such as the surgical safety checklist. Emerging digital technologies, particularly artificial intelligence (AI), may provide additional support for identifying potential safety threats during surgical care. This study evaluated the usefulness of AI-assisted monitoring for identifying and helping prevent common perioperative safety deviations in routine general surgical practice.
-
Methods
- This prospective observational study included 136 patients who underwent general surgical procedures at a tertiary hospital. Procedures included inguinal hernia repair, exploratory laparotomy, appendectomy, ventral or incisional hernia repair, excisional biopsy, and other minor surgical operations. AI-supported monitoring tools were integrated into perioperative workflows to identify potential safety deviations during operative care. Demographic characteristics, procedure types, and intraoperative safety events were recorded. The primary outcome was the frequency of safety deviations and their detection using AI support. Secondary outcomes included the proportion of identified deviations corrected before completion of surgery.
-
Results
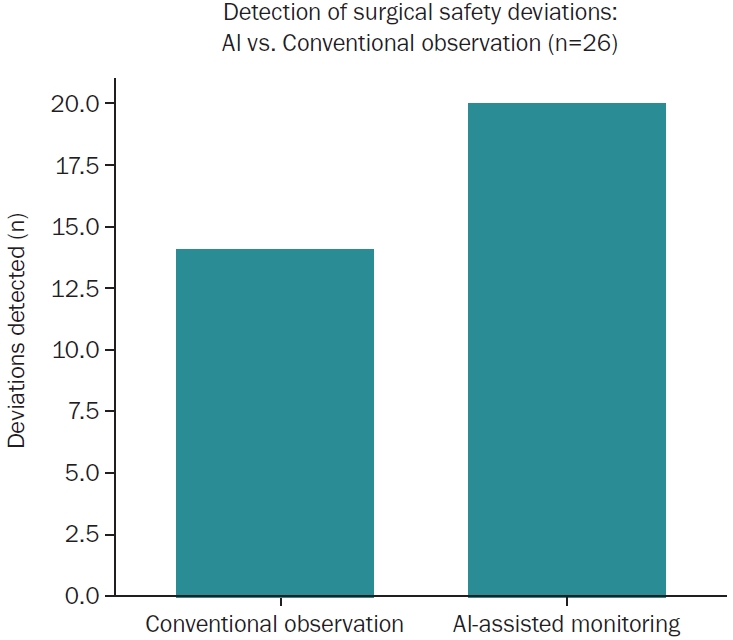
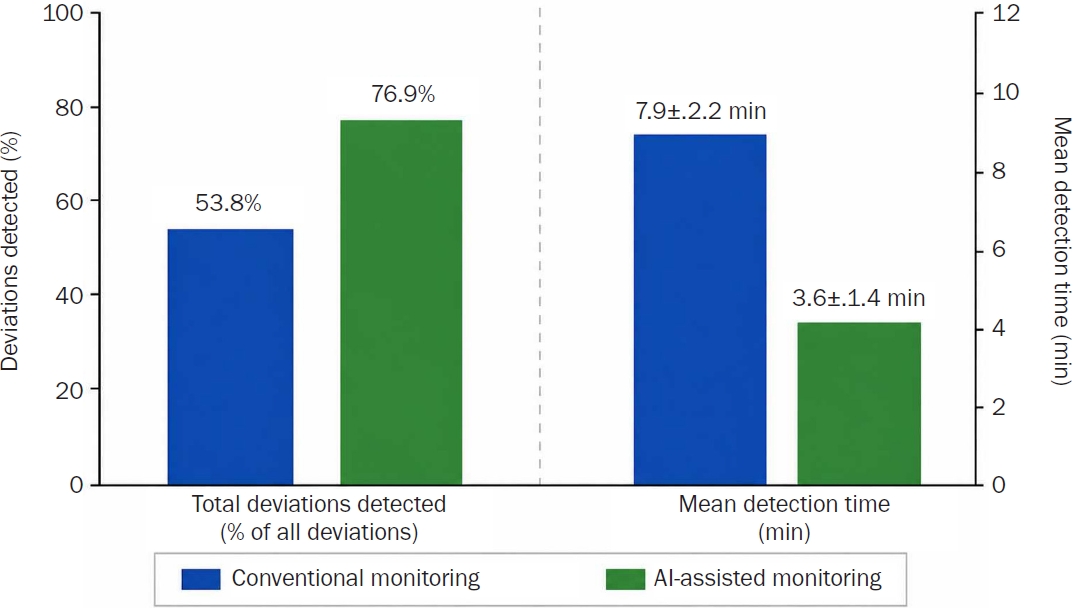
- Among the 136 procedures, 26 perioperative safety deviations (19.1%) were identified. The most common deviations involved incomplete checklist steps, delayed administration of prophylactic antibiotics, and discrepancies in instrument or sponge counts. AI-assisted monitoring detected 20 of the 26 deviations (76.9%), and 17 of the 20 detected deviations (85.0%) were corrected before completion of the procedure. The overall detection rate increased from 53.8% with routine observation alone to 76.9% with AI-assisted monitoring (p=0.02). No cases of retained surgical items or wrong-site surgery occurred during the study period.
-
Conclusions
- AI-assisted monitoring demonstrated the potential to improve early recognition and correction of perioperative safety deviations during general surgical procedures. Integration of such systems into perioperative workflows may strengthen existing safety practices and improve detection of workflow-related safety irregularities.
Introduction
Materials and Methods
Artificial intelligence-assisted monitoring and model development
Data sources
Artificial intelligence architecture
Model development
Workflow integration
Ethical safeguards
Conventional observation process and distinction from artificial intelligence-assisted monitoring
Surgical team composition and clinical experience
Data collection
Definition and categorization of perioperative safety irregularities
Checklist-performance irregularities
Antimicrobial prophylaxis timing irregularities
Surgical count inconsistencies
Documentation-related irregularities
Procedural-verification irregularities
Additional workflow-related irregularities
Results
Checklist omissions were identified in 87.5% of cases (7/8)
Antibiotic timing issues were detected in 83.3% (5/6)
Surgical count discrepancies were recognized in 80.0% (4/5)
Performance of the Monitoring System
Clarification of detection-time measurements
Intraoperative correction of Identified deviations
Completion of omitted checklist steps
Timely administration of delayed antibiotics
Verification and reconciliation of surgical counts
Correction of incomplete documentation
Discussion
Disclosure
No potential conflict of interest relevant to this article was reported.
Author contributions
Conceptualization: OQA; Data Curation: OTA, GAO, KAA, ASA; Resources: OQA, AOA, ROF; Software: OQA, ROF, ASA; Writing–original draft: OQA, AOA, AOO, KAA; Writing–review & editing: OQA, AOA, AOO, OEB, OTA, ROF, GAO, KAA, ASA, IIU.

| Category | Operational definition | Reference standard |
|---|---|---|
| Checklist-performance deviations | Incomplete, omitted, or improperly documented checklist activities during sign-in, time-out, or sign-out phases | WHO Surgical Safety Checklist [2] |
| Antimicrobial prophylaxis timing deviations | Delayed, omitted, or improperly timed prophylactic antibiotic administration before incision | WHO surgical infection-prevention guidelines [8] |
| Surgical count inconsistencies | Unresolved discrepancies involving instrument, needle, or sponge counts during operative procedures | Standard perioperative counting protocols [9] |
| Documentation-related deviations | Missing, incomplete, or inconsistent perioperative documentation or workflow records | Institutional perioperative documentation standards |
| Procedural-verification deviations | Failure or inconsistency in confirming patient identity, operative site, or intended procedure before incision | WHO perioperative verification recommendations [2] |
| Additional workflow-related deviations | Other perioperative workflow disruptions considered potentially relevant to patient safety | Institutional workflow review criteria |
| Variable | Value |
|---|---|
| Age (yr) | 43.9±14.1 |
| Sex | |
| Male | 75 (55.1) |
| Female | 61 (44.9) |
| ASA physical status classification | |
| ASA I | 39 (28.7) |
| ASA II | 68 (50.0) |
| ASA III | 29 (21.3) |
| Nature of surgery | |
| Elective | 107 (78.7) |
| Emergency | 29 (21.3) |
| Type of anesthesia | |
| General anesthesia | 82 (60.3) |
| Regional anesthesia | 34 (25.0) |
| Local anesthesia | 20 (14.7) |
| Common comorbid conditionsa | |
| Hypertension | 31 (22.8) |
| Diabetes mellitus | 14 (10.3) |
| No major comorbidity documented | 63 (46.3) |
| Primary surgical procedure | |
| Inguinal hernia repair | 40 (29.4) |
| Exploratory laparotomy | 33 (24.3) |
| Appendectomy | 25 (18.4) |
| Ventral/incisional hernia repair | 18 (13.2) |
| Excisional biopsy | 13 (9.6) |
| Other minor proceduresb | 7 (5.1) |
- 1. Makary MA, Daniel M. Medical error: the third leading cause of death in the US. BMJ. 2016;353:i2139.ArticlePubMed
- 2. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, et al. Changes in safety attitude and relationship to decreased postoperative morbidity and mortality following implementation of a checklist-based surgical safety intervention. BMJ Qual Saf. 2011;20:102-107.ArticlePubMed
- 3. Russ S, Rout S, Caris J, Mansell J, Davies R, Mayer E, et al. Measuring variation in use of the WHO surgical safety checklist in the operating room: a multicenter prospective cross-sectional study. J Am Coll Surg. 2015;220:1-11.e4.ArticlePubMed
- 4. Topol EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019;25:44-56.ArticlePubMedPDF
- 5. Hashimoto DA, Rosman G, Rus D, Meireles OR. Artificial intelligence in surgery: promises and perils. Ann Surg. 2018;268:70-76.ArticlePubMedPMC
- 6. Mascagni P, Vardazaryan A, Alapatt D, Urade T, Emre T, Fiorillo C, et al. Artificial intelligence for surgical safety: automatic assessment of the critical view of safety in laparoscopic cholecystectomy using deep learning. Ann Surg. 2022;275:955-961.ArticlePubMed
- 7. Madani A, Namazi B, Altieri MS, Hashimoto DA, Rivera AM, Pucher PH, et al. Artificial intelligence for intraoperative guidance: using semantic segmentation to identify surgical anatomy during laparoscopic cholecystectomy. Ann Surg. 2022;276:363-369.ArticlePubMed
- 8. World Health Organization. Global guidelines for the prevention of surgical site infection. WHO; 2018.
- 9. Greenberg CC, Diaz-Flores R, Lipsitz SR, Regenbogen SE, Mulholland L, Mearn F, et al. Bar-coding surgical sponges to improve safety: a randomized controlled trial. Ann Surg. 2008;247:612-616.ArticlePubMed
- 10. Anderson O, Davis R, Hanna GB, Vincent CA. Surgical adverse events: a systematic review. Am J Surg. 2013;206:253-262.ArticlePubMed
- 11. Bergs J, Hellings J, Cleemput I, Zurel Ö, De Troyer V, Van Hiel M, et al. Systematic review and meta-analysis of the effect of the World Health Organization surgical safety checklist on postoperative complications. Br J Surg. 2014;101:150-158.ArticlePubMedPDF
- 12. Esteva A, Robicquet A, Ramsundar B, Kuleshov V, DePristo M, Chou K, et al. A guide to deep learning in healthcare. Nat Med. 2019;25:24-29.ArticlePubMedPDF
- 13. Padoy N. Machine and deep learning for workflow recognition during surgery. Minim Invasive Ther Allied Technol. 2019;28:82-90.ArticlePubMed
- 14. Char DS, Shah NH, Magnus D. Implementing machine learning in health care: addressing ethical challenges. N Engl J Med. 2018;378:981-983.ArticlePubMedPMC
- 15. Rajkomar A, Dean J, Kohane I. Machine learning in medicine. N Engl J Med. 2019;380:1347-1358.ArticlePubMed
- 16. Loftus TJ, Tighe PJ, Filiberto AC, Efron PA, Brakenridge SC, Mohr AM, et al. Artificial intelligence and surgical decision-making. JAMA Surg. 2020;155:148-158.ArticlePubMedPMC
- 17. Senders JT, Arnaout O, Karhade AV, Dasenbrock HH, Gormley WB, Broekman ML, et al. Natural and artificial intelligence in neurosurgery: a systematic review. Neurosurgery. 2018;83:181-192.ArticlePubMed
- 18. Collins GS, Dhiman P, Ma J, Schlussel MM, Archer L, Van Calster B, et al. Evaluation of clinical prediction models (part 1): from development to external validation. BMJ. 2024;384:e074819.ArticlePubMedPMC
REFERENCES
Figure & Data
References
Citations
 PubReader
PubReader ePub Link
ePub Link-
 Cite this Article
Cite this Article
- Cite this Article
-
- Close
- Download Citation
- Close
- Figure
-

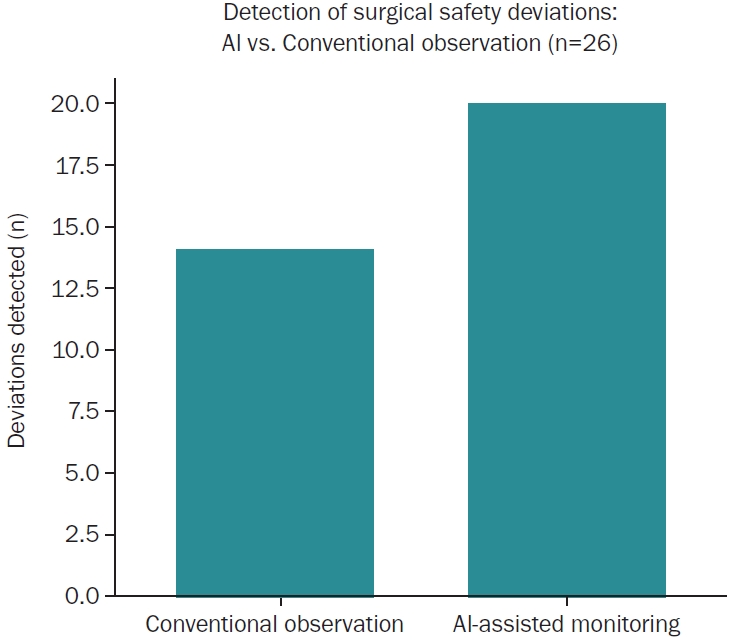
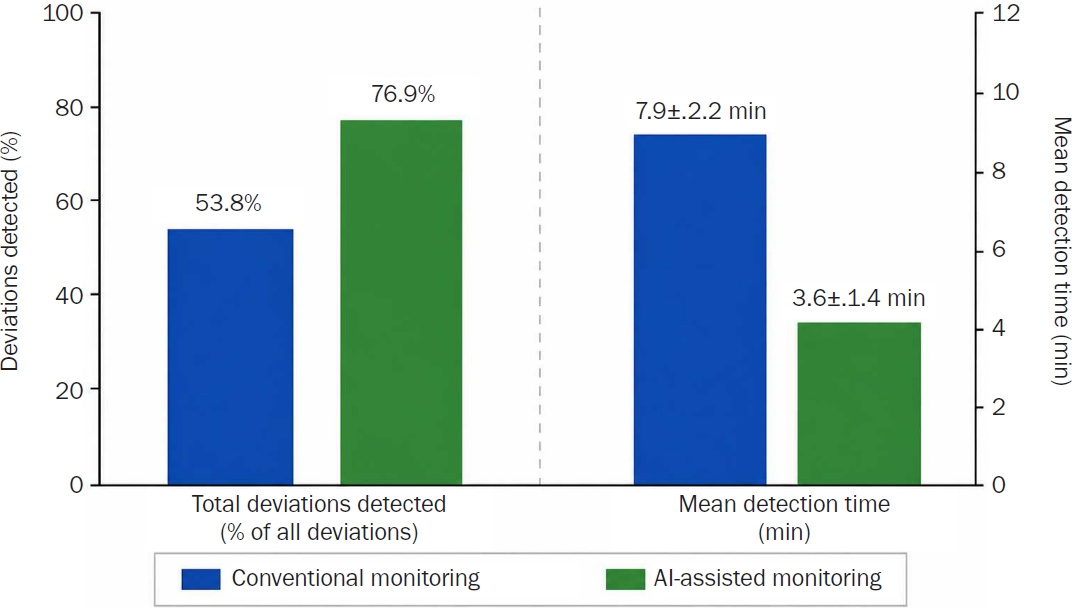

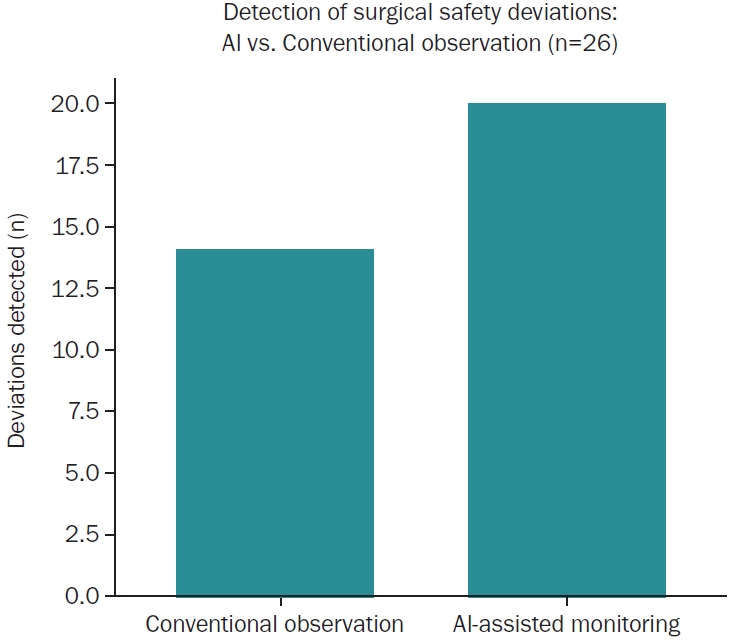
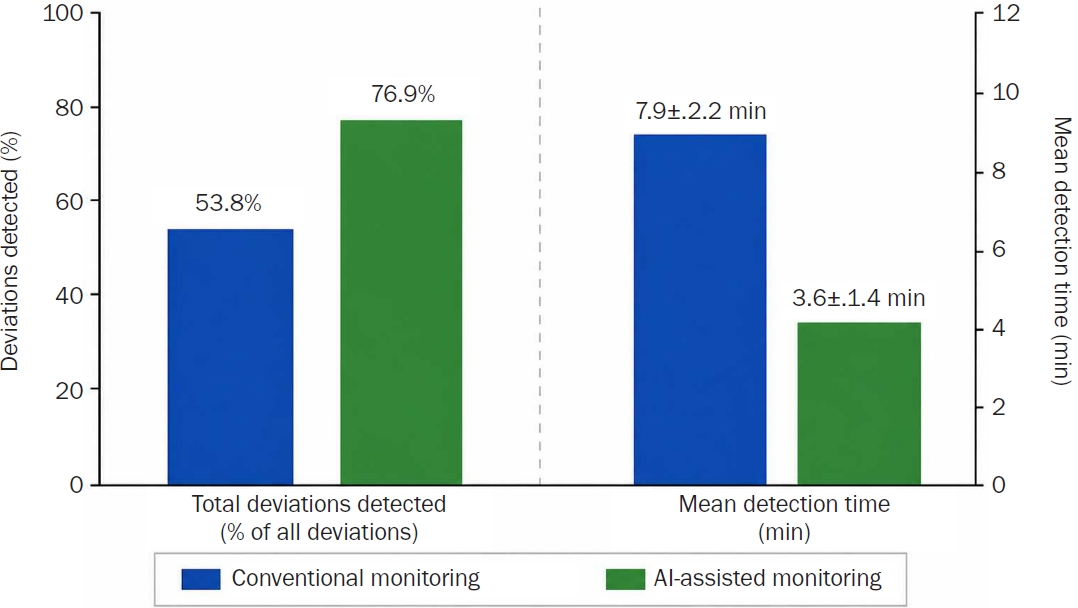
Fig. 1.
Fig. 2.
Fig. 3.
| Category | Operational definition | Reference standard |
|---|---|---|
| Checklist-performance deviations | Incomplete, omitted, or improperly documented checklist activities during sign-in, time-out, or sign-out phases | WHO Surgical Safety Checklist [2] |
| Antimicrobial prophylaxis timing deviations | Delayed, omitted, or improperly timed prophylactic antibiotic administration before incision | WHO surgical infection-prevention guidelines [8] |
| Surgical count inconsistencies | Unresolved discrepancies involving instrument, needle, or sponge counts during operative procedures | Standard perioperative counting protocols [9] |
| Documentation-related deviations | Missing, incomplete, or inconsistent perioperative documentation or workflow records | Institutional perioperative documentation standards |
| Procedural-verification deviations | Failure or inconsistency in confirming patient identity, operative site, or intended procedure before incision | WHO perioperative verification recommendations [2] |
| Additional workflow-related deviations | Other perioperative workflow disruptions considered potentially relevant to patient safety | Institutional workflow review criteria |
| Variable | Value |
|---|---|
| Age (yr) | 43.9±14.1 |
| Sex | |
| Male | 75 (55.1) |
| Female | 61 (44.9) |
| ASA physical status classification | |
| ASA I | 39 (28.7) |
| ASA II | 68 (50.0) |
| ASA III | 29 (21.3) |
| Nature of surgery | |
| Elective | 107 (78.7) |
| Emergency | 29 (21.3) |
| Type of anesthesia | |
| General anesthesia | 82 (60.3) |
| Regional anesthesia | 34 (25.0) |
| Local anesthesia | 20 (14.7) |
| Common comorbid conditions |
|
| Hypertension | 31 (22.8) |
| Diabetes mellitus | 14 (10.3) |
| No major comorbidity documented | 63 (46.3) |
| Primary surgical procedure | |
| Inguinal hernia repair | 40 (29.4) |
| Exploratory laparotomy | 33 (24.3) |
| Appendectomy | 25 (18.4) |
| Ventral/incisional hernia repair | 18 (13.2) |
| Excisional biopsy | 13 (9.6) |
| Other minor procedures |
7 (5.1) |
| Type of surgical perioperative safety deviation | Value |
|---|---|
| Incomplete surgical safety checklist steps | 8 (30.8) |
| Incorrect or delayed antibiotic prophylaxis | 6 (23.1) |
| Instrument or sponge count discrepancies | 5 (19.2) |
| Documentation errors in operative records | 4 (15.4) |
| Wrong-site/procedure verification issues | 2 (7.7) |
| Other workflow-related safety deviations | 1 (3.8) |
| Total | 26 (100) |
| Metric | Value |
|---|---|
| Sensitivity (%) | 76.9 (56.4–91.0) |
| Specificity (%) | 91.8 (84.8–96.2) |
| Positive predictive value (%) | 83.3 (62.6–95.3) |
| Negative predictive value (%) | 88.2 (80.7–93.6) |
| False-positive rate (%) | 8.2 (3.8–15.2) |
| False-negative rate (%) | 23.1 (9.0–43.6) |
| AUROC | 0.84 (0.74–0.93) |
| Classification threshold | 0.50 |
| Mean AI detection time (min) | 3.6±1.4 |
| Mean conventional detection time (min) | 7.9±2.2 |
| Variable | Conventional observation | AI-assisted monitoring | p-value |
|---|---|---|---|
| Total deviations detected | 14/26 (53.8) | 20/26 (76.9) | 0.02 |
| Mean detection time (min) | 7.9±2.2 | 3.6±1.4 | <0.001 |
| Checklist-related deviations detected | 5/8 (62.5) | 7/8 (87.5) | - |
| Antibiotic-timing deviations detected | 3/6 (50.0) | 5/6 (83.3) | - |
| Surgical-count discrepancies detected | 3/5 (60.0) | 4/5 (80.0) | - |
| Corrective actions completed before completion of surgery | 11/14 (78.6) | 17/20 (85.0) | - |
WHO, World Health Organization.
Values are presented as mean±standard deviation or number (%). ASA, American Society of Anesthesiologists. aOnly selected common comorbid conditions are presented; other comorbidities are not shown. bOther procedures included abscess drainage, lymph-node biopsy, and minor soft-tissue operations.
Values are presented as number (%).
Values are presented as estimate (95% confidence interval), threshold value, or mean±standard deviation. AI, artificial intelligence; AUROC, area under the receiver-operating characteristic curve.
Values are presented as number (%) or mean±standard deviation. AI, artificial intelligence; -, not applicable.
Table 1.
Table 2.
Table 3.
Table 4.
Table 5.
TOP

